1937-1976: War, Rights, and Hospice Origins
Interwoven themes of …
Click on images below to go to decade-specific content


1936-1946
posted in Hospice & Palliative Care Today, June 26, 2026
1. 1937–1941: The Gathering Storm
- “To establish and maintain the highest possible standards of health among the people of the United States.” ~ National Health Act of 1939
- “We cannot be a strong nation unless we are a healthy nation. And so, we must recruit not only men and materials, but also knowledge and science in service of national strength.” ~ President Franklin D. Roosevelt, on the opening of the new National Institutes of Health campus, 1940
Historical context: As the Depression dragged on, federal leaders began to say out loud that health was a national responsibility, not just a private burden or local charity. Even as war loomed overseas, they drafted surprisingly bold plans to expand public health, finance medical care, and protect those most likely to be left out.
- 1937: Technical Committee on Medical Care created to study national health needs and options for national health insurance.
- 1938: National Health Conference convenes in Washington, gathering public health officials, providers, labor, and others to debate federal responsibility for medical care and public health.
- Late 1930s: Reformers call for prepaid group practice and broader coverage as medical costs rise and access remains uneven.
- 1939: Senator Wagner’s National Health Act proposes federal funds for public health, maternal–child health, medical care for low-income people, and hospital expansion—one of the boldest pre–war attempts at a national health program.
Today’s hospice and palliative care: Today’s hospice and palliative care inherit both sides of this moment: the memory of families priced out of care, and the vision that health systems should protect the most vulnerable.
Sources: National Health Act of 1939; A (Brief) History of Health Policy in the United States; Places of Public Health: Medical Research during World War II
![]()
2. 1941-1945: America at War – Saving Lives, Counting Losses
- “December 7th, 1941—a date which will live in infamy.” ~ President Franklin D. Roosevelt, 1941
Historical context: After Pearl Harbor, the U.S. rapidly converted civilian life and medicine to a war footing, scaling up induction centers, military hospitals, and research labs. Medicine focused on keeping troops “fit to fight,” developing new ways to prevent disease, move the wounded quickly, and salvage lives that would have been lost in earlier wars.
- 1941–1945: millions of recruits processed through induction centers with medical exams, vaccinations, and classification for service.
- Battlefield medicine advances: organized forward aid stations, surgical hospitals, and evacuation chains (including growing use of air evacuation).
- Blood and fluids: shift from limited plasma early in the war to more effective products like serum albumin by 1945.
- Infection control: first large–scale combat use of penicillin and streptomycin, dramatically reducing deaths from infected wounds.
- Trauma surgery: more aggressive debridement (removal of dead tissue) lowers amputation rates compared with earlier wars.
- Morphine for the dying: medics carried morphine and basic supplies to relieve severe pain and offer as much dignity as possible in the thick of battle.
- Black Americans: more than 1.5 million Black Americans served in the military, still segregated; the “Double V” campaign—victory over fascism abroad and racism at home—advocated the belief that their military service and sacrifice should lead to full civil rights and equal access to jobs, education, and health care.
- Women: nearly 350,000 U.S. women served in the military, about 3 million worked in war plants and other defense-related jobs, and more than 19 million were in the wartime workforce overall.
- Mental health: “combat fatigue” units provide rest and removal from the front; many soldiers return to duty, but long–term psychological trauma remains underrecognized.
- Home–front hospitals: civil–defense drills, staff redeployment to the military, and wartime research projects reshape hospital routines and accelerate innovative technologies.
Today’s hospice and palliative care: Today’s hospice and palliative care are indebted to the millions whose wartime traumas pushed medicine from darkest pain and despair toward seismic shifts in compassionate care.
Sources: Take A Closer Look: America Goes to War; Medical Improvements Saved Many Lives During World War II; World War II: The African American Experience; Women in the Military During World War II
![]()
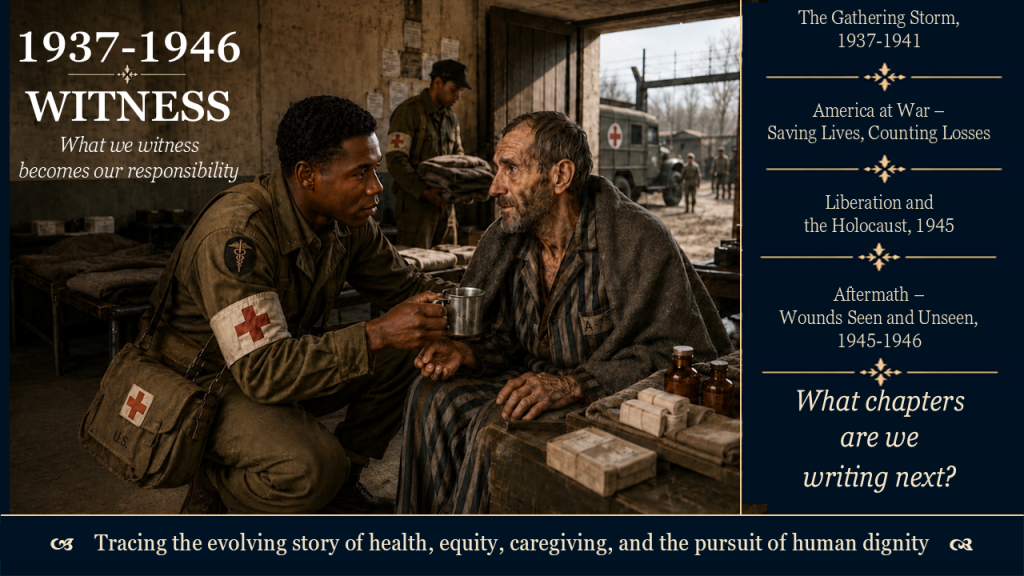
3. 1945: Liberation and the Holocaust – Witnessing the Unthinkable
- “Neutrality helps the oppressor, never the victim. Silence encourages the tormentor, never the tormented.” ~ Elie Wiesel, Holocaust survivor, 1986 Nobel Peace Prize acceptance speech
Historical context: In 1945, Allied troops liberated Nazi camps and uncovered starvation, disease, and mass killing on a scale that stunned the world. Images of skeletal Jewish survivors and mass graves exposed what happens when whole peoples are treated as less than human, even as the U.S. had turned away many Jewish refugees before and during the war.
- Camp liberations: Soldiers, medics, and chaplains entered barracks crowded with emaciated prisoners and clear evidence of systematic murder.
- Emergency care: Military medical teams scrambled to provide food, fluids, and infection control to survivors whose bodies were too fragile for standard treatment.
- Death after liberation: Many prisoners died within days or weeks, with little time or structure for emotional, spiritual, or relational care.
- Moral shock: The camps, trials, and survivor testimonies deepened the belief that every person has inherent dignity, especially when powerless and near death.
Today’s hospice and palliative care: Against this history of people deemed unworthy of rescue or refuge, hospice and palliative care insist that no one is outside the circle of care and dignity, especially those who are displaced, marginalized, or near death.
Sources: United States Holocaust Museum – Liberation of Nazi Camps; Holocaust Encyclopedia – Displaced Persons
![]()
4. 1945–1946: Aftermath – Wounds Seen and Unseen
- [Setting the stage in 1944] “We have accepted, so to speak, a second Bill of Rights under which a new basis of security and prosperity can be established for all—regardless of station, race, or creed. Among these are: … The right to adequate medical care and the opportunity to achieve and enjoy good health.” ~ President Franklin D. Roosevelt, State of the Union Address, January 11, 1944
Historical context: World War II ended with millions dead, many more living with disability and trauma, and families across the U.S. grieving. Medicine and government faced long-term responsibility for veterans’ care, not just battlefield rescue.
- Veterans Administration (VA) expansion: 1946 law creates the VA’s Department of Medicine and Surgery, formalizing a national veterans’ health system.
- Hospital demand: Returning troops and new treatments drive rising demand for hospital beds, specialists, and rehab.
- Disability and rehab: Large numbers of injured veterans spur growth in rehabilitation medicine and prosthetics, with little matching attention to emotional or spiritual needs.
- Psychological aftermath: Long-term trauma, nightmares, and moral injury are common but remain stigmatized and rarely treated.
- Families and grief: Widows, children, and parents carry heavy grief with almost no structured bereavement support.
Today’s hospice and palliative care: Born from lessons of war and its long shadows, hospices intentionally walk with aging veterans whose physical and emotional wounds have been carried for decades and into their own end-of-life care. NHPCO’s “We Honor Veterans” program was created to provide compassionate care to these “Greatest Generation” veterans from World War II and continues today for later generations of veterans, now through The Alliance.
Sources:1944 State of the Union Address Text; Object 8: Public Law 79-293, The Department of Medicine And Surgery Act, 1946; We Honor Veterans
1947-1956
posted in Hospice & Palliative Care Today, June 27, 2026
1. Hill–Burton Act and “Separate but Equal” Hospitals (1946–early 1950s)
- Every new building is also a blueprint of who is welcome inside.
Historical context: The 1946 Hill–Burton Act sparked a postwar transformation of U.S. health care infrastructure, funding a nationwide boom in hospital construction to address the severe shortage of beds after the Great Depression and World War II. It expanded capacity by helping build or modernize thousands of hospitals, nursing homes, and clinics through federal–state matching funds and required facilities to provide some free or reduced–cost care. At the same time, to secure Southern support, the law explicitly allowed “separate but equal” facilities, using public dollars to maintain racially segregated, under–resourced care for Black patients. Black physicians and civil rights advocates quickly denounced these policies as a medical civil rights issue.
Today’s hospice and palliative care: Today’s hospice and palliative care must read Hill–Burton as both achievement and warning: systems can grow and still structurally shut people out. Because of structural racism, under–insurance, and justified distrust, many Black, Hispanic, and American Indian/Alaska Native patients reach us late—through emergency departments and at advanced stages of illness. If we expand hospice and palliative care without building in equity from the start, we risk creating the next Hill–Burton—celebrated for growth, remembered for who it left out.
Sources: Hill-Burton Free and Reduced-Cost Health Care; NPR: A Bygone Era: When Bipartisanship Led To Health Care Transformation; Public Health, Racism, and the Lasting Impact of Hospital Segregation
![]()
2. Cicely Saunders, David Tasma, and the Window that Opened Modern Hospice (London, 1948)
- “I will be a window in your Home.” The promise of David Tasma of Warsaw who died 25 February 1948 and who made the first gift to St. Christopher’s Hospice
Historical context: In 1948, Cicely Saunders, then a young social worker, met David Tasma, a Polish Jewish refugee dying of cancer on a crowded London ward. His pain, loneliness, and searching conversations with her revealed how tragically standard hospital care was failing people who were dying. Before he died, he left her a small legacy with the promise, “I will be a window in your Home.” His presence—while dying—shaped her beliefs about “total pain” and became a catalyst for her journey toward creating the first modern hospice, St. Christopher’s, in 1967, in London, England.
Today’s hospice and palliative care: Tasma’s “window” invites hospice and palliative care to remember its heart: one person’s story can reshape how we care for many. Whenever a clinician pauses to be fully present in the moment, and whenever a team makes room for a patient’s story to guide the plan, that “window” reveals how clearly we see those we serve, and humanity in our larger world.
Sources: Dame Cicely Saunders; St. Christopher’s plaque of David Tasma’s Window
![]()
3. From Home Death to Hospital Death (early mid 1950s)
- Death moved from the home to the hospital, and the machines kept watch.
Historical context: By the 1950s, antibiotics, complex surgeries, and early ventilators had turned hospitals into high–tech centers of acute care. Death, once most often at home, increasingly took place in hospital wards and nursing homes, where clinicians could intervene longer and more aggressively, reshaping how families and communities experienced dying.
Today’s hospice and palliative care: This move from home death to hospital death handed medicine powerful tools but also a culture of prolonging dying in ways that can deepen suffering. Hospice and palliative care stand at this crossroads, using hospital care to ease distress, clarify what matters most, and, whenever possible, help people spend their final days in ways that are truly person–centered—shaped by their own values, relationships, and preferred places of care.
Sources: History of Hospitals; World Health Organization – Palliative
1957-1966
posted in Hospice & Palliative Care Today, June 28, 2026
1. 1950s – Baby Boomers and the Promise of a Longer Life
- By 2030, all baby boomers will be age 65 or older.
Historical context: Postwar America celebrated survival and science. Antibiotics, the Salk polio vaccine, and expanding hospitals meant more children grew up and more adults lived longer. The Baby Boom (1946–1964) swelled the future elder population, while nursing homes and chronic–care facilities quietly expanded. Few grasped how many people would someday live for years with dementia, multimorbidity, and frailty.
Today’s hospice and palliative care: We now meet that vast generation of Baby Boomers as “Senior Boomers.” Longer life has become a stress test: rising elder census and healthcare needs, workforce shortages, and caregiver strain all trace back to those mid–century gains. Today’s hospice and palliative care is helping redesign care for this aging majority—scaling home–based serious–illness care, supporting exhausted caregivers, and advocating for health systems and families to plan for predictable late–life living and dying.
Sources: Baby boom | Definition, Cause, & Facts; Hospice in America by the Numbers – 2026; The 2030 Problem: Caring for Aging Baby Boomers
![]()
2. 1963 – President John F. Kennedy’s Death and Televised Grief
- CBS TV News Bulletin: “From Dallas, Texas, the flash, apparently official. President Kennedy died at 1:00 p.m. Central Standard Time, 2:00 Eastern Standard Time, some 38 minutes ago.” ~ Walter Cronkite, November 22, 1963
Historical context: President John F. Kennedy’s assassination in 1963 turned grief into a shared national broadcast. Continuous television coverage carried images of shock and ritual into living rooms, while millions sent condolence letters to a family they had never met. A largely private experience became a collective, media–shaped event, revealing how deeply people needed language, witness, and participation after traumatic loss.
Today’s hospice and palliative care: This national crisis echoed the 1865 death of President Abraham Lincoln and foreshadowed how we mourn now: publicly, visually, and often online. Hospice and palliative teams can respond by creating intentional spaces for shared remembrance—memorials, story circles, digital rituals—and by helping families limit re–traumatizing exposure to images and coverage. Looking ahead, our work is to treat grief as both personal and communal, asking “Where is your loss being seen?” and shaping supports that reach beyond the solitary individual into community and digital life.
Source: YouTube – CBS TV News Bulletin, Walter Cronkite; NPR: How live TV helped America Mourn The Loss of JFK
![]()
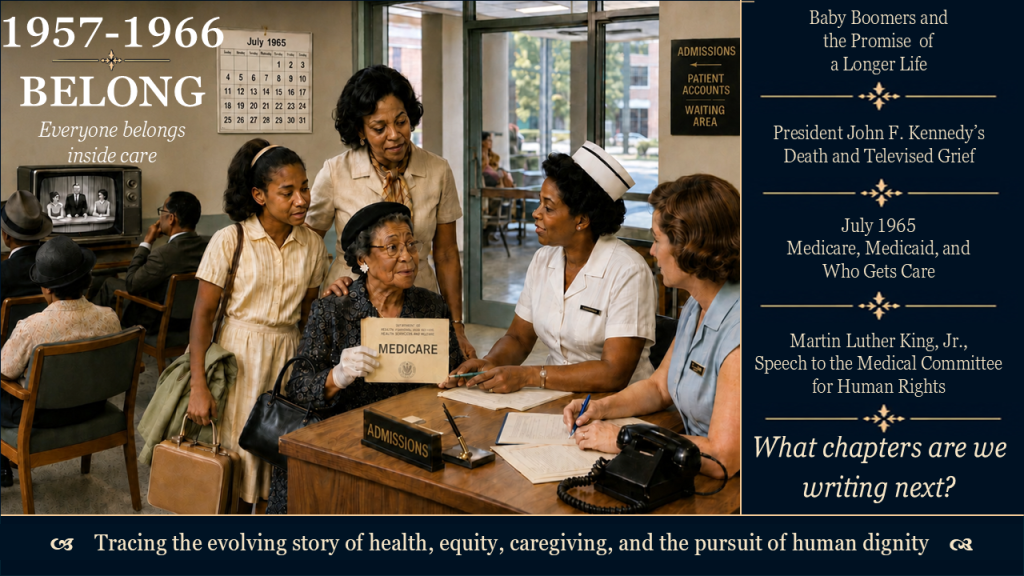
3. 1965 – Medicare, Medicaid, and Who Gets Care
- “No longer will older Americans be denied the healing miracle of modern medicine.” ~ President Lyndon B. Johnson at the signing of the Medicare and Medicaid Act, July 30, 1965
Historical context: In 1965, Congress created Medicare and Medicaid, tying hospital and medical care for older and low–income Americans to federal law. Overnight, elders gained significant coverage, and Medicaid became the main safety net for nursing–home care. Two decades before “hospice” was a formal benefit, this legislation laid the financial tracks on which most late–life and end–of–life care in the United States runs, today.
Today’s hospice and palliative care: Since 1966, more than 160 million people have been entitled to Medicare, and today nearly 2 in 5 Americans are covered by Medicare or Medicaid—a scale that makes these programs the backbone of serious–illness and end–of–life care in the United States. This reach is both gift and warning: hospice depends on these funds even as quality gaps, fraud, and long–standing inequities threaten public trust. Our task is to use this architecture for justice—strengthening integrity and equity so that care reaches those who have historically been left out.
Sources: President Lyndon B. Johnson’s Remarks on the Medicare Bill; National Archives – Medicare and Medicaid Act (1965); Medicare and Medicaid by the Numbers – 60th Anniversary, 2025
![]()
4. Martin Luther King Jr., speech to the Medical Committee for Human Rights, March 25, 1966
- “Of all the forms of inequality, injustice in health is the most shocking and the most inhuman because it often results in physical death.” ~ Dr. Martin Luther King, Jr.
Historical context: The 1946 Hill-Burton Act supported segregated hospitals. The landmark Civil Rights Act of 1964 outlawed discrimination based on race, color, religion, sex, or national origin. In theory, it ended segregation in public places and employment. In March 1966, speaking with the Medical Committee for Human Rights in Chicago, Dr. King named health care as a frontline of injustice.
Today’s hospice and palliative care: King’s words still test us. Hospice and palliative programs that overlook race, poverty, language, disability, or geography risk repeating the inequities he condemned. The call now is concrete and hopeful: know who is being missed, listen with communities at the margins, and shape policy and practice so that comfort, communication, and support at the end of life are signs of justice, not privilege.
Sources: Getting Martin Luther King’s words right; Dr. Martin Luther King on health care injustice
1967-1976
posted in Hospice & Palliative Care Today, June 29, 2026
1. A world watching death, injustice, and possibility
- “Each time a man stands up for an ideal or acts to improve the lot of others or strikes out against injustice, he sends forth a tiny ripple of hope.” ~ Robert F. Kennedy
Historical context: In these few years, a new generation watches death, injustice, and wonder unfold in real time.
- Vietnam War body counts appear nightly on television, making distant deaths immediate and political.
- The assassinations of Martin Luther King Jr. and Robert F. Kennedy bring sudden public grief and deepen racial and political fractures.
- Civil rights, Black Power, and antiwar movements expose hidden violence and demand dignity for marginalized communities.
- College and teen rebellions challenge institutional authority, including how medicine handles truth, suffering, and dying.
- The Apollo 11 moon landing becomes a shared global triumph, expanding imaginations about what humanity can do together.
Into this contested landscape step Cicely Saunders, Elisabeth Kübler-Ross, and Florence Wald, each offering a different way to insist that every dying person is, in Robert F. Kennedy’s words, “a human being whom other human beings loved and needed,” and should be cared for accordingly.
Today’s hospice and palliative care: These years still echo in today’s headlines—war, racial violence, protest, and breakthrough science all shape what people expect at the end of life. The question is whether hospice and palliative care will look away, or offer truthful, humane care that centers those most exposed to harm. Continue reading to see how three visionary leaders reimagined care for people who are dying—and why their work still matters now.
Sources: Robert F. Kennedy Quotes; History.com
![]()
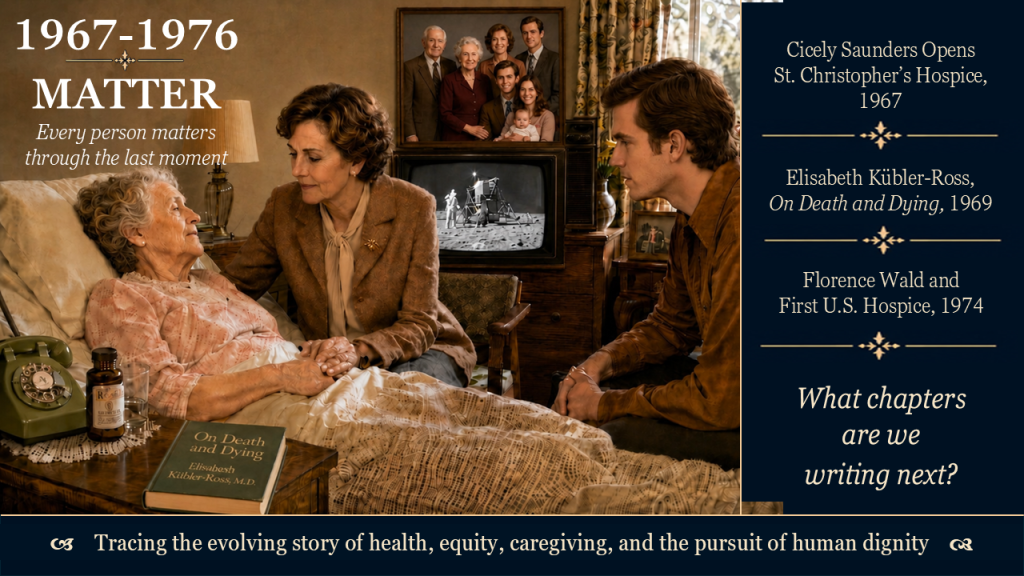
2. 1967, Dame Cicely Saunders opens St. Christopher’s, the first modern hospice
- “You matter because you are you, and you matter to the last moment of your life; and we will do all we can not only to help you die peacefully, but also to live until you die.” ~ Cicely Saunders
Historical context: In 1967, Dr. Cicely Saunders opens St. Christopher’s Hospice in London as a radical alternative to hidden, medicalized dying. She brings together meticulous pain and symptom control, attention to family and story, and a commitment to research and teaching. Hospice becomes a place where clinical precision and human presence are not opposites but partners.
Today’s hospice and palliative care: Saunders’ words still cut through noise and burnout. Her vision challenges us to treat pain, fear, and isolation as urgent equity issues, not optional extras. For teams and leaders, the question is simple and searching: what would it look like here—for this patient to “live until they die”?
Source: Cicely Saunders International; Cicely Saunders Quotes
![]()
3. 1969, Elisabeth Kübler-Ross authors On Death and Dying
- “People are like stained-glass windows. They sparkle and shine when the sun is out, but when the darkness sets in, their true beauty is revealed only if there is a light from within.” ~ Elizabeth Kübler-Ross
Historical context: While a generation watches death on their screens and protest in their streets, Dr. Elizabeth Kübler-Ross sits at the bedside, listens, and lets patients speak for themselves. Her work makes public what many already know: that people facing death want honesty, conversation, and connection, not secrecy and sedation. Her book On Death and Dying introduces the famous “five stages” language into public conversation.
Today’s hospice and palliative care: Grief clinicians no longer treat grief as “stages.” Still, she opened the door to talking about the silenced thoughts “death and dying.” She affirmed that emotions near the end of life are real, varied, and worth hearing. Her legacy invites clinicians to move beyond delivering “bad news” toward ongoing, two-way conversations.
Sources: Biography – Dr. Elizabeth Kübler-Ross; Elisabeth Kübler-Ross: “People are like stained-glass windows …”
![]()
4. Florence Wald, founder of the first U.S. hospice, 1974
- “We need to cure sometimes, but care always.” ~ Florence Wald
Historical context: In 1963 Florence Wald—then dean at Yale School of Nursing—attended a lecture by Cicely Saunders and later studied with her in England. She eventually left academic leadership to build a model that combines home care, a free-standing hospice, family involvement, and team-based support for people who are dying. Hospice becomes, in her words, the “end piece” of a continuum of care, not a sign of medical failure. This first hospice in America opened in 1974, Connecticut Hospice in Branford.
Today’s hospice and palliative: Wald’s “care always” lives on through the remembered dying and grief experiences for the millions of hospice patients and families served across the United States since1974. Her “care always” sharply confronts today’s systems ruined by fraud. Her legacy pushes us to start palliative conversations earlier, center home and community-based care, and bring hospice principles into places where people still die with little support. The question for leaders today is not whether hospice belongs in the U.S. system, but whether it will remain a peripheral service or become a standard of care wherever serious illness and dying unfold.
Sources: Connecticut Women’s Hall of Fame; Connecticut Hospice – History; Death with Dignity: 50th Anniversary of America’s First Hospice