1776-1866: Founding and Fracture
Interwoven themes of “All are created equal,” Early United States, Healthcare of Soldiers, Epidemics, Slavery, Early Medical Education, Early Public Health, and Civil War
Click on images below to go to decade-specific content

1776-1786
Posted in Hospice & Palliative Care Today, June 10, 2026
1. Continental Congress, Declaration of Independence, July 4, 1776
- “We hold these truths to be self-evident, that all men are created equal, that they are endowed by their Creator with certain unalienable Rights, that among these are Life, Liberty and the pursuit of Happiness.” Thomas Jefferson, principal drafter for the Continental Congress
Historical context: Adopted by the Second Continental Congress, the Declaration’s assertion of equality and human rights provided the moral language later used by abolitionists, reformers, disability-rights advocates, public-health leaders, and hospice and palliative care voices arguing for the dignity of every person. In a care-centered timeline, this is the foundational American claim that every life possesses worth.
Today’s hospice and palliative care: Rights to dignity, access to care, core respect for each other (patients, families, staff, volunteers, leadership, community).
Sources: National Archives, https://www.archives.gov/founding-docs/declaration-transcript
![]()
2. Dr. Benjamin Rush, Directions for Preserving the Health of Soldiers, 1778
- “The art of preserving the health of a soldier consists in attending to the following particulars.” Dr. Benjamin Rush, physician, Continental Army medical leader, signer of the Declaration of Independence
Historical context: Rush’s pamphlet was the first American public health manual focused on preventive medicine and military hygiene, articulating principles — clean water, proper food, adequate rest — that predated germ theory by a century. Rush is often called the “Father of American Psychiatry” and advocated for humane treatment of the mentally ill at a time when such individuals were routinely jailed.
Today’s hospice and palliative care: Preventive medicine leads to longer life expectancy. Infection control. Caregiver wellness.
Source: The American Revolution Institute, “Benjamin Rush’s Directions for Preserving the Health of Soldiers”
1787-1796
Posted in Hospice & Palliative Care Today, June 11, 2026
1. Dr. Benjamin Rush, letter to Reverend Richard Allen, September 1793
- “It has pleased God to visit this city with a malignant and contagious fever, which infects white people of all ranks, but passes by persons of your color.” ~ Dr. Benjamin Rush, the only signer of the Declaration of Independence with a medical degree, advocated for humanization of psychiatric treatment
- Reverend Richard Allen, born into slavery 1760 and purchased his freedom. Prolific preacher. Co-founder of the African Methodist Episcopal Church (AME).
Historical context: During Philadelphia’s catastrophic 1793 yellow fever epidemic — which killed approximately 5,000 of the city’s 51,000 inhabitants — physician Rush asked Black Philadelphians to remain in the city and serve as nurses and undertakers, based on the erroneous medical belief that Black people were immune. Black Philadelphians who stayed and served did, in fact, die from the fever at significant rates.
Today’s hospice and palliative care: Prevention of discrimination to patients and employees. Evidence-based research paired with clinical best practices and ethics.
Source: American Journal of Public Health, “A Contemporary Black Perspective on the 1793 Yellow Fever Epidemic”
![]()
2. Absalom Jones & Richard Allen, A Narrative of the Proceedings of the Black People, Philadelphia, 1794
- “We have suffered equally with the whites, our distress hath been very great, but much unknown to the white people.”
- Absalom Jones, born into slavery in 1746, learned to read, purchased freedom for his wife and himself. Co-founded the Free African Society with Richard Allen. Established the St. Thomas African Episcopal Church in Philadelphia, the first Black Episcopal congregation in America.
- Reverend Richard Allen, born into slavery 1760 and purchased his freedom in the early 1780’s. Prolific preacher. Co-founder of the African Methodist Episcopal Church (AME).
Historical context: During the catastrophic 1793 Philadelphia yellow fever epidemic, free Black Philadelphians — led by Jones and Allen — answered the city’s call to nurse the sick and bury the dead, believing (mistakenly) that they had immunity. Their 1794 pamphlet, the first copyrighted work by African Americans, stands as the founding document of Black civic health witness in America.
Today’s hospice and palliative care: Core, inclusive healthcare. Evidence-based research paired with clinical best practices and ethics. Emergency disaster management. Workplace safety. Infection control. Employee rights and responsibilities.
Sources: A Narrative of the Proceedings of the Black People During the Late Awful Calamity in Philadelphia (1794); A Contemporary Black Perspective on the 1793 Yellow Fever Epidemic in Philadelphia – PMC
![]()
3. United States Congress, An Act Relative to Quarantine, 1796
- “An Act Relative to Quarantine,” Adopted by the Third Congress and signed by George Washington
Historical context: One of the earliest federal public health statutes, the Quarantine Act established that the federal government had a role in protecting the public from epidemic disease — a foundational precedent for all subsequent public health law in the United States. The act was passed in response to the recurring yellow fever epidemics that devastated port cities in the 1790s. More comprehensive federal quarantine law in 1799, “Act Respecting Quarantines and Health Laws.”
Today’s hospice and palliative care: COVID 19. Centers for Disease Control and Prevention (CDC).
Source: Library of Congress Law Blog: An Act Relative to Quarantine (1796) – Statutes and Stories
1797-1806
posted in Hospice & Palliative Care Today, June 12, 2026
1. United States Congress / President John Adams, Act for the Relief of Sick and Disabled Seamen, July 16, 1798
- “[Congress established a fund] to provide treatment for sick and injured merchant seamen.” United States Congress; signed by President John Adams
Historical context: The Act for the Relief of Sick and Disabled Seamen created the Marine Hospital Service, the direct predecessor of the U.S. Public Health Service, and is widely regarded as the first federal healthcare program in America. It levied a mandatory payroll deduction of twenty cents per month from merchant seamen’s wages to fund hospital care, establishing the principle of contributory public health financing 167 years before Medicare.
Today’s hospice and palliative care: Today’s U.S. Public Health Service. Veterans Administration hospitals.
Sources: U.S. National Library of Medicine, History of PHS; Marine Hospice Service formally renamed US Public Health Service (1912); NIH Images – Health Care for Seamen
![]()
2. Enslaved Healers and Midwives — Care in the Cabins, Early 1800’s
- Often practicing in the privacy of their cabins, enslaved people drew on their knowledge of local flora and healing practices to make medicines and provide care, … much of it with roots in West African traditions. … Enslaved women played a particularly powerful role in enslaved communities as healers and midwives. … Black people … tended to the mental and emotional health of their families as well, a need that white doctors and overseers did not bother with.
Historical Context: Enslaved women and men used African and local botanical knowledge to tend the sick, deliver babies, and comfort the dying in slave quarters across the South. Their unacknowledged expertise underwrote a parallel system of end-of-life care built on mutual aid and resilience, in sharp contrast to a legal system that treated them as property and offered no formal protection in illness or death. And, upon learning of their expertise, some white owners prohibited their access to the plants used to bring comfort and healing.
Today’s hospice and palliative care: Long history of inequitable systems for healthcare medicines, timely and affordable care, and (until recent decades) medical employment.
Sources: Medical Care and the Health of Enslaved People; Herbal Use by Enslaved Africans
![]()
3. Home Deaths at the Turn of the 19th Century (Late 1700’s-Mid 1800’s)
- Women who cared for the dying were called ‘watchers’ or ‘watchwomen.’ People died at home. Family members, typically the women, cared for their loved one’s body (i.e., bathed and dressed for burial).
Historical Context: For white North Americans, death was expected to happen in one’s own bed, surrounded by kin, with clergy and neighbors moving in and out of the sickroom. Women in families and communities were the ones who sat up through the night, watched for changes in breathing, offered sips of water, and prayed at the bedside. There were little formal medical interventions at the end of life and no funeral industry. Instead, communities relied on customs, faith, and women’s caregiving skills to accompany the dying and tend the dead.
Today’s hospice and palliative care: The American hospice movement returned care to the “home” death. This “home preference” frames much hospice marketing, today. The gender gap among caregivers has been closing. Still, recent research shows expectations for daughters to provide more care than sons.
Sources: When Death Was Women’s Work; Death and Dying in North America, Late 18th–19th Century; Study Who Cares for Mom and Dad? The Sibling Divide in Caregiving
![]()
4. Home Parlors and Funerals at the Turn of the 19th Century (Late 1700’s-Mid 1800’s)
- Once a person died, they were bathed by either family or servants and laid out in their best clothes so their loved ones could say one last goodbye. … The body would then be laid out and displayed at home, in the parlor if the house had one, or even on the dining table.
Historical Context: Family and neighbors washed and dressed the body, kept watch, and laid out the body for a period of 1-3 days. This time of final “watching” and of family “Wakes” helped ensure that the person had indeed died. Strong smelling flowers such as lilies were often used to hide smells of decomposition. The deceased person was carried to and buried at a nearby family or church plot. Death was close, visible, and woven into daily life.
Today’s hospice and palliative care: The “Wake” moved to funeral homes and more recently has been shifting to “Celebration of Life” venues. Today’s common cremation practices significantly changed practices of viewing the body, timing, location, and more. Today’s “green burials” are growing as environmentally friendly options.
Sources: Remembering a Life—‘From Parlors to Slumber Rooms’; Grave decisions: Understanding attitudes and perceptions towards green burial — A review of literature
1807-1816
posted in Hospice & Palliative Care Today, June 13, 2026
1. Francis Scott Key, ‘The Star-Spangled Banner,’ September 14, 1814
- “O’er the land of the free and the home of the brave.”
Historical context: Key’s line emerges from a moment of wartime crisis, linking national survival with military sacrifice and an ideal of freedom—voiced in a nation still shaped by slavery. In O Say Can You Hear: A Cultural Biography of “The Star Spangled Banner,” Mark Clague traces how the anthem’s meaning has evolved across two centuries. As The National Endowment for the Humanities notes, Clague argues that the anthem reflects the nation’s ongoing effort to become “a more perfect union.” Read. Learn. Sing it with fresh understanding.
Today’s hospice and palliative care: In today’s hospice and palliative care, “freedom” gets very personal—deciding goals of care, where someone wants to die, and putting advance directives in place within the bounds of the law. It also brings tougher questions: what “freedom” means when a mother’s life is at risk in a perinatal crisis, or when considering medical aid in dying (MAiD). And “brave” is shifting too. Instead of “fighting a battle,” we’re talking more about living as fully as possible—and, when the time comes, peacefully letting go.
Sources: Smithsonian National Museum of American History, lyrics PDF; The Star Spangled Music Foundation; National Endowment for the Humanities
![]()
2. Dr. Daniel Drake, Natural and Statistical View, or Picture of Cincinnati, 1815
- “The diseases of this country are modified by the climate, the soil, the state of society, and a variety of local causes… [The] poor settler’s family, exposed to all the vicissitudes of the climate, without comfortable lodging, and with a scanty, often unwholesome diet, is peculiarly liable to every species of disease.” ~ Dr. Daniel Drake (1785-1852), physician and founder of medical education in the American Midwest; founder of the Cincinnati School of Medicine
Historical context: Daniel Drake, a leading frontier physician and medical educator in Cincinnati and Louisville, was one of the first American physician voices to frame illness and mortality as shaped by climate, housing, poverty, and “the state of society”—not just individual bodies. Writing amid high mortality among women, infants, and children, and life expectancy often between 20 and 40 years, he insisted on bedside and hospital-based training grounded in lived conditions, helping shift medical understanding toward what we now call the social determinants of health.
Today’s hospice and palliative care: We continue Drake’s insight that place matters. Bedside teaching and interdisciplinary training remain central. Local and national data—from CMS, NHPCO/The Alliance, and Hospice Analytics—help map serious illness “hot spots” and guide equity efforts. Social workers and care teams translate social risks into care plans, extending this place-based lens to hospice access, experience, and outcomes.
Sources: About Daniel Drake; Indiana University Lilly Library commentary on Drake’s medical geography work; Natural and Statistical View, or Picture of Cincinnati (1815)
![]()
3. Almshouses as Places to Die — Poor Relief and Separation
- From the late seventeenth century to the early twentieth century, almshouses offered food, shelter, clothing, and medical care to the poorest and most vulnerable, yet often in exchange for hard labor and forfeiture of freedom.
Historical context: By the early 1800s, almshouses had become the default destination for people who were poor, chronically ill, mentally ill, or without family support. Many died there, far from home. Care and containment were intertwined, as communities struggled to meet complex needs with limited medical knowledge and caregiving resources.
Today’s hospice and palliative care: Then—almshouses blurred care and containment. Now—care focuses on person-centered comfort, dignity, and goals of care across homes, senior living, assisted living, and skilled nursing facilities. Medicaid, Medicare, and nonprofit and philanthropic support expand access—including for those unable to pay. Still, “who dies where” is shaped by insurance coverage, medication costs, access, rural gaps, workforce shortages, and cultural and language barriers. Emerging models, including prison hospice, continue to extend compassionate end-of-life care.
Sources: Philadelphia Encyclopedia — Almshouses/Poorhouses; Poor Relief and the Almshouse
1817-1826
posted in Hospice & Palliative Care Today, June 14, 2026
1. New York City Common Council laws regulating funerals of enslaved persons
- 1722, with increasingly restrictive laws and informal practices nationwide
- For the preventing of great numbers of slaves assembling and meeting together at their Funerals, … it was ordered that, if more than twelve slaves assembled at a slave funeral, those present were to be whipped at the discretion of the Mayor, Recorder or one of the Alderman except the 12 slaves admitted by the owner of the dead slave, the gravedigger and the corpse bearers.
Historical context: Such American legislation began as early as 1680 among colonists, seeking to eliminate any rituals, music, beliefs related to enslaved persons’ homeland; seeking to control. Among a few of the many restrictions (with variations): specific hours for burials that often conflicted with enforced work hours; numbers of persons (as in the example above); the funeral had to be led by a white priest or preacher; no singing, drumming, dancing (culturally important rituals); no use of palls (the cloth covering the casket or body, hence “pallbearer”); and more. Over time, African American funerals became known as “home-goings,” as in being released from suffering and the soul either returning to Africa or going to heaven. Black spirituals that grew out of suffering and prayer became signals for the Underground Railroad: “Wade in the Water,” “Steal Away,” “Swing Low Sweet Chariot.”
Hospice and palliative care today: Attend a vibrant, full-of-love Black funeral in America today, and you will likely experience a deep sense of community, emotion, storytelling, formal greetings from other Black communities of faith, and music! A lot of music. The burial may be accompanied by a solemn jazz band processional, followed by a “second line” New Orleans-style community celebration when leaving.
Sources: Homegoing; Harriet Tubman Historical Society; New Orleans Second Line History; Music of the Soul – Composing Life Out of Loss
![]()
2. Dr. Benjamin Rush, Medical Inquiries and Observations, Volume I (4th edition, published posthumously in 1815 and actively circulated in medical schools during this period)
- “The customs of civilized life have given rise to a great number of diseases, which are unknown in savage and barbarous nations.” ~ Benjamin Rush
Historical context: Benjamin Rush—signer of the Declaration of Independence—remained an influential medical voice decades later, as his widely circulated work shaped early American medical education. Yet his legacy is deeply conflicted. During Philadelphia’s 1793 yellow fever epidemic, he urged Black residents to remain and serve as nurses and undertakers, based on the false belief that they were immune—reinforcing patterns of racial exploitation and harm. At the same time, his writings advanced an early recognition that the conditions of “civilized” life—its habits, environments, and inequities—could themselves produce disease.
Today’s hospice and palliative care: Rush’s era exposed a tension we still carry—equality is proclaimed, yet care is marked by bias and exclusion. Hospice care is growing more honest about that legacy by tracking disparities, building trust, and confronting its own blind spots. Many professionals name the “moral distress” they experience when ethics collide with unequal systems. Many organizations are doing crucial work to close that gap.
Sources: Medical Inquiries and Observations, Volume I (4th ed., 1815) – National Library of Medicine digital collection; A Contemporary Black Perspective on the 1793 Yellow Fever Epidemic in Philadelphia
![]()
3. American School for the Deaf, Hartford, Connecticut, April 15, 1817
- The founding of the American School for the Deaf in Hartford, Connecticut, in 1817 was a crucial milestone in the way society related to people with disabilities.
Historical Context: On April 15, 1817, the Connecticut Asylum for the Education and Instruction of Deaf and Dumb Persons, later renamed the American School for the Deaf, opened in Hartford with seven students. As the first permanent school for deaf children in the United States, it helped establish American Sign Language, Deaf education, and a durable Deaf community and culture.
Today’s hospice and palliative care: This entry offers a hopeful reminder that care is not only clinical treatment; it is also communication, belonging, dignity, and social inclusion. For hospice and palliative care, the ongoing lesson is that people who communicate, perceive, age, grieve, or suffer differently deserve systems designed to meet them where they are, not systems that define them by exclusion.
Source: American School for the Deaf: History & Cogswell Heritage House
1827-1836
posted in Hospice & Palliative Care Today, June 15, 2026
1. Dr. Thomas Percival, Medical Ethics published 1803 in England and circulating in American medical education during this timeframe
- “The feelings and emotions of the patients under critical circumstances require to be known and to be attended to, no less than the symptoms of their diseases.”
Historical context: Though British in origin, Percival’s Medical Ethics became a foundational source for American medical ethics. The American Medical Association’s 1847 Code of Ethics drew heavily on Percival’s Medical Ethics. Its insistence that patients’ feelings matter alongside symptoms anticipates the humane, whole-person approach that modern hospice and palliative care would later describe more fully.
Today’s hospice and palliative care: Percival’s principle is an early ethical ancestor of palliative care’s attention to the whole person, including fear, grief, distress, family concerns, and meaning. In today’s hospice and palliative care, excellent care requires more than treating symptoms. It requires listening for the emotional, relational, and existential suffering that patients and families carry under “critical circumstances.”
Source: American Medical Association Code of Ethics History (Ochsner Journal, 2003)
![]()
2. U.S. Congress, Indian Removal Act, 1830; Cherokee Nation Memorial, 1829, on the Eve of the Trail of Tears
- Cherokee Nation plea to Congress upon threats of removal: To the land of which we are now in possession we are attached, it is our father’s gift, it contains their ashes, it is the land of our nativity, and the land of our intellectual birth. 1829
- Congressional Indian Removal Act: An Act to provide for an exchange of lands with the Indians residing in any of the states or territories, and for their removal west of the river Mississippi. 1830
- The soldiers came and took us from home. … The drove us out of doors and did not permit us to take anything with us, not even a second change of clothes. … They marched us, … even our little children …” Oo-la-cha, widow of Sweet Water, as told in 1842, The Trail Where They Cried
Historical context: In December 1829, Cherokee leaders and citizens petitioned Congress against removing them from their homeland. They described their homeland not simply as property, but as the land of their birth and death, from generation to generation to generation. Still, Congress passed the Indian Removal Act the following year, signed by President Andrew Jackson, beginning a broader removal era that affected many Native nations, including the Choctaw, Muscogee/Creek, Chickasaw, Seminole, and Cherokee. The Cherokee forced removal of 1838-1839 became the event most specifically remembered as the Trail of Tears, but the suffering reached across multiple peoples and homelands for generations. Oo-loo-cha’s 1842 testimony gives human voice to that history: families were not merely “removed”; they were stripped of their dignity, homes, possessions, children’s safety, ancestors’ graves, and places where life and death had meaning.
Today’s hospice and palliative care: This history reminds us that grief can be communal, ancestral, cultural, and tied to place. In hospice and palliative care today, cultural humility requires us to truly hear generational stories of injustice, spirituality, rituals, roles, language needs, land connections, and sources of mistrust that may shape illness, dying, remembrance, and care. That humility matters for Native patients and families whose histories long predate the United States, and for patients, families, and staff from many nations and languages who may carry displacement, trauma, or sacred traditions we do not yet understand, but are called to meet with wise care.
Sources: Cherokee Nation Memorial to Congress, 1829; U.S. Congress, Indian Removal Act, 1830; Oo-loo-cha, as told in 1842; The Trail of Tears and the Forced Relocation of the Cherokee Nation, National Park Service; President Andrew Jackson’s Message to Congress “On Indian Removal,” National Archives; End-of-Life Care Disparities Experienced by American Indian and Alaska Native Peoples, Journal of Palliative Medicine, 2025; Healing with Humility: Palliative Care for Refugee Communities, American Journal of Nursing, 2026
![]()
3. Narrative of Frederick Douglass, an American Slave, 1845; describing c. 1833-1835
- “I was broken in body, soul, and spirit. My natural elasticity was crushed, my intellect languished, the disposition to read departed, the cheerful spark that lingered about my eye died; the dark night of slavery closed in upon me; and behold a man transformed into a brute!”
Historical context: Douglass wrote this passage describing the physical and psychological destruction wrought on his body and mind by the slave-breaker Edward Covey, who beat Douglass repeatedly when Douglas was about 15-17 years old. This passage is one of the clearest first-person accounts in American literature of how slavery deliberately attacked human health, dignity, intellect, and spirit as instruments of control.
Today’s hospice and palliative care: Douglass’s words reveal suffering as assaults on a person’s whole humanity: body, soul, spirit, intellect, and hope. For hospice and palliative care today, this calls us to more than comfort; it calls us to trauma-informed care that restores dignity, listens without defensiveness, and recognizes how histories of dehumanization still shape trust, access, fear, and the care people need at life’s most vulnerable thresholds.
Sources: Narrative of the Life of Frederick Douglass, an American Slave (1845), Chapter X
1837-1846
posted in Hospice & Palliative Care Today, June 16, 2026
1. Joseph Warrington’s Nurse Society of Philadelphia, 1839, “This Room Holds Life and Death”
- “To engage in the important business of nursing mother and child in the lying–in chamber…” [the bedroom where a woman labored and recovered after childbirth]
Historical context: In 1839, Quaker physician Joseph Warrington helped organize the Nurse Society of Philadelphia, training working–class women to care for mothers and infants in their own homes during childbirth and the precarious days after delivery. These nurses entered cramped back bedrooms where poverty, infection, and hemorrhage meant that birth and death were close neighbors, and their work included recognizing danger, comforting families, and keeping vigil when a mother or newborn was dying. Warrington’s Nurse’s Guide named women’s bedside tasks—watching, washing, soothing, staying—as skilled labor that mattered at the boundary between life and death and in the first hours of grief, when the room held both a body and a stunned family.
Today’s hospice and palliative care: Today, pregnancy and birth still carry real risks, especially in rural and under–resourced communities where maternity units have closed and emergency transfers are long. Mothers still die from complications of pregnancy and childbirth, and whole families live with grief from miscarriages, stillbirths, and the loss of infants after high–risk births. Perinatal and pediatric palliative care teams now walk with parents when a fetus, newborn, or child has a life–limiting condition, and grief counselors tend these especially painful losses. At the bedside—whether in a home or a small rural hospital—hospice team members continue Warrington’s work when they stay present in the delivery space that has become a deathbed, help parents hold and bless a baby who has died, and make sure no one faces that grief alone.
Sources: Joseph Warrington, The Nurse’s Guide (1839); American Nursing: An Introduction to the Past
![]()
2. Oliver Wendell Holmes Sr., “The Contagiousness of Puerperal Fever,” 1843
- “The woman about to become a mother, or with her new-born infant upon her bosom, should be the object of trembling care and sympathy wherever she bears her tender burden or stretches her aching limbs… God forbid that any member of the profession to which she trusts her life, doubly precious at that eventful period, should hazard it negligently, unadvisedly, or selfishly!”
Historical context: In 1843, Boston physician Oliver Wendell Holmes Sr. argued that puerperal (childbed) fever often was carried from one woman to another on the unwashed hands and instruments of doctors—turning birthbeds into deathbeds through preventable infection. His essay, later reissued with an even sharper preface in 1855, accused the profession of killing new mothers at horrifying rates and demanded that physicians stop moving directly from autopsies and infected patients to the delivery room without cleansing themselves or their tools. Preceding Semmelweis’s work in Vienna, Holmes’s fury at this obstetric violence was a landmark in medical ethics and an early step toward germ theory, insisting that respect for mothers required strict attention to how clinicians’ own bodies and instruments transmitted disease.
Today’s hospice and palliative care: Holmes’s warning puts today’s common infection–control practices into an ethical framework, grounded in the hard outcomes of maternal and infant deaths. Safety culture, hand hygiene, PPE, and other infection–control measures now shape basic care so that people near the end of life are less likely to be harmed by the very hands meant to help them. We saw similar excruciating deaths during COVID–19 when infections ravaged health throughout hospitals, nursing homes, and households.
Source: Oliver Wendell Holmes (1809–1894) and his essay on puerperal fever
![]()
3. Dorothea Dix, Petition for the Mentally Ill to the Legislature of Massachusetts, January 1843
- “I proceed, Gentlemen, to call your attention to the present state of Insane Persons confined within this Commonwealth, in cages, closets, cellars, stalls, pens… I come to present the strong claims of suffering humanity…”
Historical context: In 1843, reformer Dorothea Dix carried a searing report to the Massachusetts legislature after visiting jails, almshouses, and poorhouses where people with mental illness were chained, beaten, left naked in cold cells, and abandoned without treatment. Her petition described lives pushed toward early death and what we might now call social death—people cut off from family and community, suffering and dying unseen. By insisting that those hidden in “cages” and “pens” deserved warmth, safety, and care at the end of life, Dix turned private horror into public responsibility and helped spark a movement for state hospitals that, at its best, was meant to replace degradation with basic comfort.
Today’s hospice and palliative care: Dix’s witness challenges us to ask who is still suffering and dying “out of sight” today. Hospice and palliative teams now work in settings for the unhoused, mentally ill, incarcerated, and under–resourced communities to bring pain and symptom relief, companionship, and spiritual care. When we problem-solve services for the unhoused, for psychiatric patients’ access to palliative consults, for hospice beds behind bars, or other similar suffering, we carry forward Dix’s conviction that the measure of a society is found in whether anyone is willing to see, name, and stand beside those whom others would prefer to lock away and forget.
Sources: Dorothea Dix, “Memorial to the Legislature of Massachusetts” (1843), The American Yawp Reader
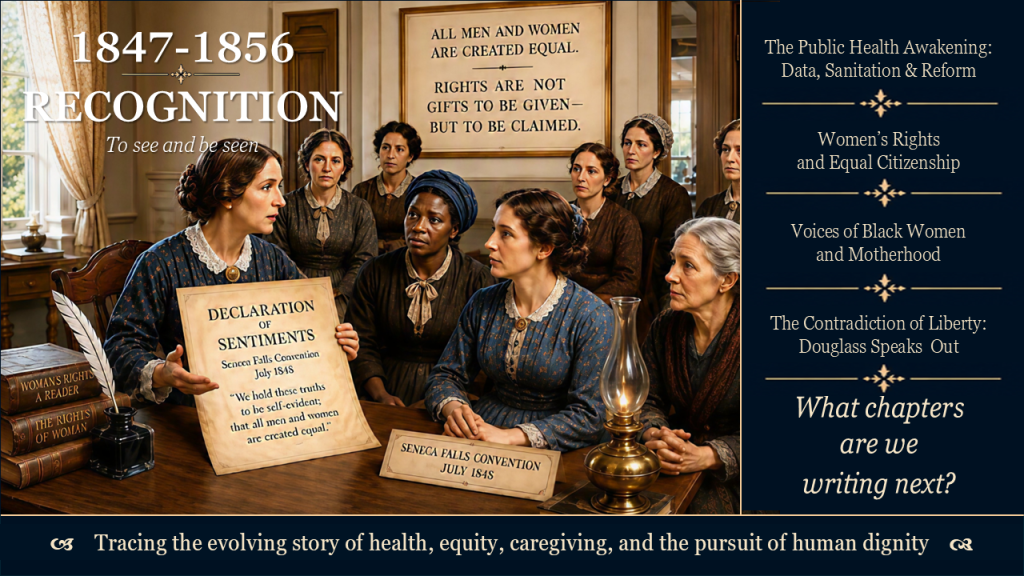
1847-1856
posted in Hospice & Palliative Care Today, June 17, 2026
1. Lemuel Shattuck, Report of the Sanitary Commission of Massachusetts, 1850
- “The conditions which now surround a large portion of the population, especially in cities and large towns, and sometimes also in smaller towns and rural districts, are clearly unfavorable to health; and the reform which is now needed demands the attention of the government, the physician, and the philanthropist.”
Historical context: Lemuel Shattuck (1793–1859) was a statistician and public health reformer. His 1850 report marked the first systematic American use of birth and death records to describe population health and the first attempt to articulate a comprehensive public health code. Written when life expectancy in Boston was approximately 25 years, it explicitly linked poverty, overcrowding, and inadequate sanitation to preventable death.
Today’s hospice and palliative care: Shattuck showed, with data, that poor living conditions lead to preventable illness and early death—and that addressing them is a public responsibility. Building on earlier physicians like Daniel Drake and working alongside reformers like Dorothea Dix, he demonstrated that where and how people live shapes who suffers and dies—and that this demands a public response. This carries forward into hospice and palliative care’s focus on inequity, social determinants, and the responsibility to care at and beyond the bedside.
Sources: Report of a General Plan for the Promotion of General and Public Health (1850); Internet Archive
![]()
2. Elizabeth Cady Stanton and delegates of the Seneca Falls Convention,
Declaration of Sentiments, July 1848
- “We hold these truths to be self-evident; that all men and women are created equal.”
Historical context: The Declaration of Sentiments deliberately echoed the Declaration of Independence to expose women’s exclusion from the political and civic promises of 1776. By naming equality for “men and women,” the Seneca Falls Convention located women’s rights within the nation’s ongoing argument over liberty, consent, bodily autonomy, and citizenship.
Today’s hospice and palliative care: This claim that women’s lives and choices carry equal moral and civic weight undergirds contemporary commitments to respect autonomy in serious illness. In hospice and palliative care, it strengthens the insistence that women’s voices, bodies, caregiving burdens, and end-of-life decisions deserve the same authority, protection, and dignity as men’s within families, systems, and law.
Sources: “Declaration of Sentiments,” National Park Service, Women’s Rights National Historical Park
![]()
3. Sojourner Truth, Ohio Women’s Rights Convention, Akron, 1851 (as recorded by Frances Dana Gage, 1863)
- “I have borne thirteen children, and seen most all sold off to slavery, and when I cried out with my mother’s grief, none but Jesus heard me! And ain’t I a woman?” ~ Sojourner Truth
Historical context: Sojourner Truth, born into slavery in New York, delivered this speech against arguments that women were too delicate to claim rights, answering instead with her enslaved life of hard labor, repeated childbearing, and the sale of her children. The speech stands as a foundational document of Black maternal suffering, naming the forced sale of children as a grief uniquely borne by enslaved women in a nation that claimed to honor motherhood.
Today’s hospice and palliative care: Sojourner Truth’s testimony names a mother’s grief that was both deeply personal and created by slavery’s laws and violence. Her question, “Ain’t I a woman?” shows how race and gender shape whose pain is believed and whose motherhood is honored—and whose is not. For hospice and palliative care, her voice calls us to recognize disenfranchised suffering and loss, and to make sure that people’s traumatic stories and grief are fully heard, valued, and woven into how we understand and respond to their present struggles.
Source: Speech at the Ohio Women’s Rights Convention, Akron, Ohio [National Park Service]
![]()
4. Frederick Douglass, “What to the Slave is the Fourth of July?” Rochester,
New York, July 5, 1852
- “The sunlight that brought life and healing to you, has brought stripes and death to me. This Fourth of July is yours, not mine. You may rejoice. I must mourn.” ~ Frederick Douglass
Historical context: Douglass delivered this speech thirteen years after escaping slavery, addressing a largely white audience gathered in Rochester to commemorate Independence Day. By pairing “life and healing” with “stripes and death,” he used the language of the body to name the contradiction of a nation that celebrated liberty while permitting the ongoing violence, illness, and early deaths of enslaved people.
Today’s hospice and palliative care: Douglass’s contrast between “life and healing” for some and “stripes and death” for others’ names people whose enslavement and suffering were ignored even as the nation celebrated freedom. Read alongside Cicely Saunders’s insistence, “You matter because you are you,” and her claim that “approaches to death and dying reveal much of the attitude of society as a whole.” Paired together, their words call hospice and palliative care to ask where we are truly embodying equal regard—and where our approaches to death and dying still inflict avoidable suffering and reveal attitudes that some lives and losses matter less.
Sources: “What to the Slave is the Fourth of July?” Rochester, New York; [National Constitution Center]; Saunders’ quotes in Foreword in The Oxford Textbook of Palliative Medicine. Oxford University Press, Oxford (1993)
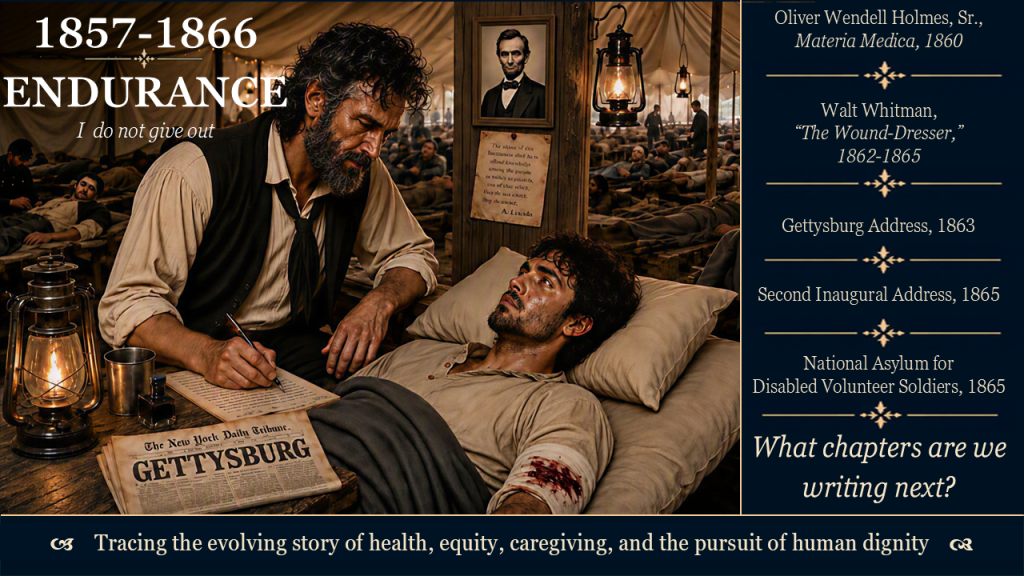
1857-1866
posted in Hospice & Palliative Care Today, June 18, 2026
1. Dr. Oliver Wendell Holmes, Sr., Annual Meeting of the Massachusetts Medical Society, 1860
- “I firmly believe that if the whole materia medica, as now used, could be sunk to the bottom of the sea, it would be all the better for mankind — and all the worse for the fishes.”
Historical context: On the eve of the Civil War, Oliver Wendell Holmes, Sr.—Boston physician and Dean of Harvard’s Medical School—warned his colleagues that many popular drugs and treatments did more harm than good. He called for restraint and evidence rather than blind faith in the “materia medica” (pharmacology).
Today’s hospice and palliative care: His 19th-century skepticism foreshadowed today’s concerns about polypharmacy and futile interventions near the end of life.
Sources: Baylor University Medical Center Proceedings: Medical and Surgical Care During the American Civil War
![]()
2. Walt Whitman, “The Wound-Dresser,” written from his wartime nursing experience 1862-1865
- “I am faithful, I do not give out, The fractur’d thigh, the knee, the wound in the abdomen, These and more I dress with impassive hand, (yet deep in my breast a fire, a burning flame.) I sit by the restless all the dark night, some are so young, Some suffer so much, I recall the experience sweet and sad.” ~ Walt Whitman
Historical context: After his brother was wounded at Fredericksburg, Walt Whitman spent three years as a volunteer nurse in Washington, D.C. military hospitals during the war, writing letters for dying soldiers and dressing wounds. “The Wound-Dresser” is his poetic record of those experiences and a central literary document of American nursing care from the Civil War era, told from the caregiver’s perspective.
Today’s hospice and palliative care: Whitman’s “wound-dresser” shows what care looks like when cures are few: steady hands, night-long presence, and attention to bodies that are “so young” and “suffer so much.” His poem gives hospice and palliative care an early language for the quiet work of sitting at the bedside, witnessing pain, and finding something “sweet and sad” in staying faithful to the wounded and dying rather than turning away.
Sources: “The Wound-Dresser,” Drum-Taps (1865); Biography – Walt Whitman(1819-1892); Medical and surgical care during the American Civil War, 1861–1865
![]()
3. President Abraham Lincoln, Gettysburg Address, November 19, 1863
- “Four score and seven years ago our fathers brought forth on this continent, a new nation, conceived in Liberty, and dedicated to the proposition that all men are created equal… that this nation, under God, shall have a new birth of freedom — and that government of the people, by the people, for the people, shall not perish from the earth.”
Historical context: Delivered at the dedication of the Soldiers’ National Cemetery at Gettysburg, where thousands of dead were reburied after the battle of July 1–3, 1863, this address reshaped how Americans understood mass death and national sacrifice.
Today’s hospice and palliative care: At Gettysburg, Lincoln asked a grieving nation to face mass death and respond with a “new birth of freedom,” not only with monuments and memory. His words resonate with hospice and palliative care’s long work of bereavement: walking with people whose losses may never fully heal, yet whose inconsolable sorrows can be honored, carried, and sometimes turned toward new purpose beyond the grave.
Sources: Abraham Lincoln Online, The Gettysburg Address (Bliss copy); Cornell University’s Transcript
![]()
4. President Abraham Lincoln, Second Inaugural Address, March 4, 1865
- “With malice toward none, with charity for all, with firmness in the right as God gives us to see the right, let us strive on to finish the work we are in, to bind up the nation’s wounds, to care for him who shall have borne the battle and for his widow and his orphan.”
Historical context: Two years after Gettysburg (July 1863), with the war nearly over and the toll of suffering clearer, Lincoln’s second inaugural named a national duty “to care for him who shall have borne the battle, and for his widow and his orphan,” a line later adopted as the official motto of the Department of Veterans Affairs.
Today’s hospice and palliative care: This call to “bind up the nation’s wounds” echoes in modern hospice and palliative care for veterans, their families, and survivors of war. It reminds clinicians and systems that serious illness, disability, and bereavement among those who served are not just private tragedies, but shared obligations of the community and the state.
Source: National Park Service, “With Malice Toward None”:
![]()
5. United States Congress, Act Establishing the National Asylum for Disabled Volunteer Soldiers, signed by President Abraham Lincoln, March 1865
- Congress created the National Asylum for Disabled Volunteer Soldiers
Historical context: One of Lincoln’s last acts of legislation before his April 1865 death, the National Asylum for Disabled Volunteer Soldiers — later renamed the National Home for Disabled Volunteer Soldiers — was the first large-scale federal institution dedicated specifically to the long-term care of disabled veterans, inaugurating the principle of government responsibility for those injured in national service. By 1873, Congress had also established pension programs and a home-nursing aid program for disabled veterans unable to care for themselves.
Today’s hospice and palliative care: This act stands at the root of today’s veteran-focused care, such as NHPCO/The Alliance’s widespread “We Honor Veterans” programs, which recognize the ongoing impact of military service at the end of life. Today, hospice and palliative care teams put into action that caring for veterans means honoring their service and addressing war’s lasting physical, emotional, and moral wounds for both veterans and their families.
Sources: Journal of the Civil War Era, “Caring for Veterans: The Civil War and the Present”; We Honor Veterans
Leave a Reply
You must be logged in to post a comment.